

Background: Traditionally, intensive induction chemotherapy has been the primary front-line treatment for AML; however, older adults are often poor chemotherapy candidates and as of 2009, nearly 50% of older AML patients did not receive any treatment (Mederios, Ann Hematol 2015). Recently, several non-traditional front-line AML regimens have emerged, including hypomethylating agents (HMA), the BCL-2 inhibitor venetoclax, liposomal anthracycline and cytarabine, and targeted therapies. These non-traditional agents may offer less intense side effects and provide novel front-line options for older adults. We hypothesized the advent of non-traditional options has allowed a greater proportion of older adults to receive effective treatment, thereby improving survival for this population. Using a population-based approach, we evaluated front-line treatment patterns and outcomes of older adults with AML in the modern era.
Methods: Patients ≥ 60 years with a first diagnosis of AML in the California Cancer Registry (CCR) between 2014-2017 were included. Front-line regimen was manually abstracted from unstructured free-text fields in the CCR. The CCR was linked with California's Patient Discharge Database (PDD) to obtain hematopoietic cell transplantation (HCT) information. Multivariable logistic regression examined factors associated with front-line treatment regimen and multivariable Cox proportional hazards regression examined factors associated with survival.
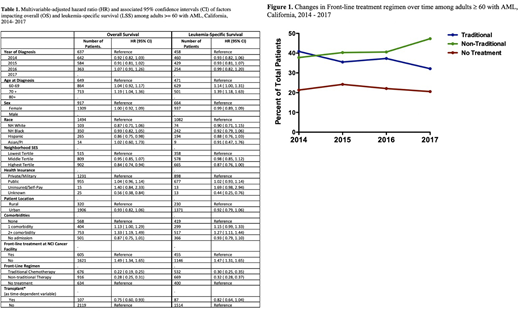
Results: Of the 4,086 patients identified, 3,068 (75%) had sufficient treatment information to classify front-line regimen and are included; 34% were 60-69 years at diagnosis, 39% were 70-79, and 27% were ≥ 80. Thirty-three percent received front-line therapy at an NCI-designated cancer center and 12% received HCT. The median follow-up time was 121 days. Across the time period studied, 36% received traditional cytotoxic chemotherapy, 42% received non-traditional therapy, and 22% received no treatment. Of the patients receiving traditional therapy, 84% received cytarabine plus anthracycline. Of those receiving non-traditional therapy, 85% received HMA monotherapy, 8% HMA plus venetoclax, and 3% liposomal cytarabine plus anthracycline. Use of both non-traditional therapy and HCT increased over time, with 38% of patients receiving non-traditional therapy in 2014 vs 47% in 2017 (p < 0.001) and 8.4% of patients receiving HCT in 2014 compared to 11.1% in 2017 (p < 0.001.) The proportion of patients not receiving treatment did not change significantly over time, with 23% in 2014 vs 24% in 2017 (p = 0.20).
Multivariable analyses (MVA) revealed receipt of treatment was significantly associated with age < 80 (p < 0.001), < 2 comorbidities (p < 0.001), and receipt of front-line therapy at an NCI-designated cancer center (p < 0.001). Compared to traditional chemotherapy, non-traditional frontline therapy was associated with age ≥ 80 (p < 0.001) and ≥ 2 comorbidities (p = 0.001). Race/ethnicity, socioeconomic status, and type of insurance were not associated with receipt of treatment or type of front-line regimen.
One-year overall survival (OS) of the full cohort was 25% (CI: 23.6 - 26.5%). One-year OS was 44% (CI: 40.8 - 47.1%) for patients receiving traditional chemotherapy, 31.4% (CI: 40.8 - 47.13%) for patients receiving non-traditional therapy, and 4.38% (CI: 2.73 - 6.04%) for patients who were not treated. The MVA for OS demonstrated age ≥ 80 (HR 1.19, CI 1.04 - 1.36), ≥ 2 comorbidities (HR 1.33, CI 1.19 - 1.49), and not receiving front-line therapy at an NCI cancer center (HR 1.49, CI 1.34 - 1.65) to be independently associated with inferior OS; receipt of traditional chemotherapy (HR 0.22, CI 0.19 - 0.25) and HCT (HR 0.75, CI 0.6 - 0.93) were associated with superior OS.
Conclusion
Using a population-based approach, we show the patterns of care for AML treatment in older adults is changing, with an increasing proportion of patients receiving both initial treatment and HCT relative to historical reports and a significant increase in the use of newer, non-traditional therapies. Similarly, survival estimates are improving over time for patients who receive therapy. During our study period, a significant proportion of older adults with AML remain untreated, which is strikingly impacted by location of front-line care. At the population level, there remain opportunities to increase access to therapy for older adults with AML.
Muffly:Amgen: Consultancy; Servier: Research Funding; Adaptive: Research Funding.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal